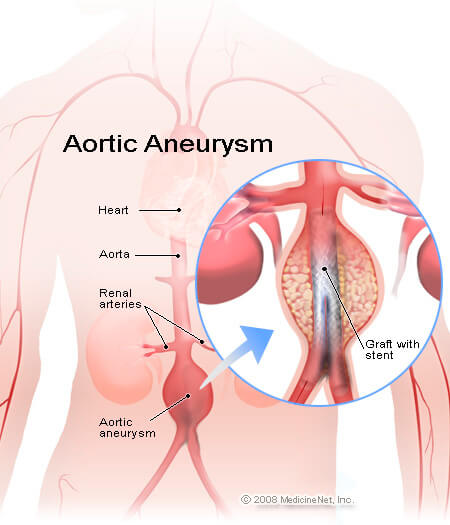
Abdominal Aortic Aneurysm
The aorta is the major blood vessel that supplies blood to the body. An abdominal aortic aneurysm (AAA) is an enlarged and weakened area in the lower part of the wall of the aorta. A normal aorta is approximately one inch or less in diameter and it runs from the heart passing through the center of the chest and abdomen. In general, aneurysms can develop anywhere along the length of an aorta. Aneurysms in the upper part of the aorta are called thoracic aortic aneurysms. But, aneurysms are more common in lower parts of an aorta and called as abdominal aortic aneurysms. These aneurysms may also be referred to as AAA or triple-A.
An aneurysm can grow to be more than five inches in diameter. Due to a high pressure of blood flowing through the artery, the weakened area enlarges like a balloon. It is more common to see large aneurysms bursting as compared to the smaller ones.
This results in internal bleeding that can lead to death unless treated immediately by an experienced cardiovascular surgeon. AAAs are considered a serious health condition because they can burst or rupture. Only about half of patients with a ruptured AAA who get to a hospital survive. Treatment of AAA may vary from watchful waiting to emergency surgery depending on the size and rate at it is growing. Once a diagnosis of AAA is made, doctors will closely monitor it so that surgery can be planned if it’s necessary. It is very risky to wait for surgery until the time AAA ruptures.
9,600+
Happy Patients
10
Qualified Doctors
500+
Successful Surgeries
100+
Insurance Partners
There are several tests your doctor may order to help confirm whether you have angina:
Aneurysms of the aorta are more common in the abdominal part of aorta. The exact cause of abdominal aortic aneurysms is unknown, but various factors may play a role, which includes:
Abdominal aortic aneurysms are mostly slow growing and have no symptoms. This makes them difficult to detect. Some aneurysms will never rupture. Many aneurysms are small to begin with and stay small, although many expand over time. Some expand quickly. It is very difficult to predict how fast an abdominal aortic aneurysm may enlarge.
Enlargement of an abdominal aortic aneurysm may lead to:
Any person who is a smoker or aged 60 years or more, with a family history of abdominal aortic aneurysm is at risk of developing an abdominal aortic aneurysm. He/she should consider regular screening for the condition. As male sex, as well as smoking, has preponderance for abdominal aortic aneurysm, men ages 65 to 75 who have ever smoked cigarettes should have a one-time screening for abdominal aortic aneurysm using abdominal ultrasound.
Regular screening for people at risk of abdominal aortic aneurysms
Several medical bodies active in preventive medicine recommend that men aged 65 to 75 who have ever smoked should have a one-time screening for abdominal aortic aneurysm using abdominal ultrasound. The need for a screening ultrasound should be discussed with doctors by people older than age 60 with a family history of abdominal aortic aneurysm or other risk factors.
The main complication of abdominal aortic aneurysm is tears in the wall of the aorta (dissection). Life-threatening internal bleeding can ensue of an AAA ruptures. The risk of rupture is greater in large aneurysms.
Signs and symptoms indicating that aortic aneurysm has burst are:
Development of blood clots is another complication of aortic aneurysms. Small blood clots can develop in the area of the aortic aneurysm. A loose clot that breaks away from the wall of an aneurysm can block a blood vessel elsewhere in the body, causing pain or blocking the blood flow to the legs, toes, kidneys or abdominal organs.
Treatment of AAA is very specific. Some general guidelines for treating abdominal aortic aneurysms are:
Small-sized aneurysm
In case of a patient having a small abdominal aortic aneurysm — about 1.6 inches, or 4 centimeters (cm), in diameter or smaller — and without symptoms, the doctor may suggest a watch-and-wait (observation) approach, rather than surgery. Surgery, in general, isn’t needed for small aneurysms because the risk of surgery likely outweighs the risk of rupture. If a patient chooses the observation approach, the doctor will monitor the aneurysm with periodic ultrasounds, usually every six to 12 months and encourage the patient to report immediately if there is abdominal tenderness or back pain — potential signs of a dissection.
Medium-sized aneurysm
The size of a medium aneurysm is between 1.6 and 2.1 inches (4 and 5.3 cm). How the risks of surgery versus waiting stack up in the case of a medium-size abdominal aortic aneurysm, is unclear. The benefits and risks of waiting versus surgery will need to be discussed with the doctor and then an informed decision be made with the help of the doctor. In case of watchful waiting, an ultrasound will be needed every six to 12 months to monitor the aneurysm size.
Large, fast-growing or leaking aneurysm
Surgery is generally required in cases of an aneurysm that is large (larger than 2.2 inches, or 5.6 cm) or growing rapidly (grows more than 0.5 cm in six months). Additionally, a leaking, tender or painful aneurysm requires treatment.
For abdominal aortic aneurysms, two types of surgeries are available:
Lifestyle
Lifestyle measures are the best approach to prevent an aortic aneurysm as they keep the blood vessels as healthy as possible. That means taking these steps:
In case somebody has any of the risk factors for aortic aneurysm, it is very important to talk to the doctor. If you are at risk, your doctor may recommend additional measures. These include medications to lower blood pressure and relieve stress on weakened arteries.